It was a lovely day last Sunday to Massage at Apperley’s quarter marathon.
Couldn’t have asked for a nicer day after Saturday being so wet and windy. Met some familiar faces and some new ones which I look forward to having sessions with over the coming weeks. A well done to all the runners, organisers and marshals for a well ran event.
As England steam rollered Sri Lanka recently and have now started on Pakistan I felt it was a good time to have a look into cricketers and the most common injuries they face. (The less said about the football the better really)
Bowling, especially fast bowling is the most common movement to pick up an injury. The most likeliest place to get injured from this movement is the back.
It is likely that the bowler’s injury will be down to overuse, therefore it is important for the coaches during training to monitor the amount of bowling. Its also from pertinent for the captain of the team in matches to regularly switch bowlers to make sure each one is at a much reduced risk of getting an overuse injury.
Previous injury is seen as a very good indictor for current injuries in a fact bowler as it has been shown that once they get an injury it is very likely to reoccur. This is where it is very important for healthcare professionals to look at all predisposing factors for an injury.
The most common example of this is to look at the hips/back. If a player’s back is lordotic, then this will cause the pelvis to tilt forward, this then elongates the hamstrings and puts them on stretch. With the hamstrings being in such a way this exposes the player to an increased risk of a hamstring strain. If a player picks up a hamstring strain and the therapist does not alter any of the above then it is more likely for the player to repeatedly receive hamstring strains as the predisposing factors which put the body at risk of the injury in the first place.
The second most common position for injury is fielding. This is seen to be due to the demands of diving for catches. There has even been an increase in ‘whiplash’ injuries in the C spine (shoulders to head area) from the impact of diving and landing to catch the ball, regaining balance and then quickly throwing the ball back.
The younger cricketer with an age of around 17 years old is the most at risk of being injured. This is thought to be down to the fact their bodies are still growing and their bodies find it harder to keep up with the training and match demands.
Two thirds of injured cricketers in the study were able to return to matches and training session with one week of being out. This is a marked decrease in time as two decades ago it would have been twice as long.
For more information on this and where my points came from please see the below Journals
Clarsen, B., & Bahr, R. (2014). Matching the choice of injury/illness definition to study setting, purpose and design: one size does not fit all!. British journal of sports medicine, 48(7), 510-512.
Stretch, R. A. (2003). Cricket injuries: a longitudinal study of the nature of injuries to South African cricketers. British Journal of Sports Medicine, 37(3), 250-253.
Last week I had a client and during the session I said to them ‘these exercises will help improve proprioception’ the client then asked ‘what actually is proprioception!? I’ll do the exercises but I don’t know why!
After I had explained a bit about it all and why it matters, it occurred to me how many times I have actually been asked that question, therefore I’m going to delve a bit deeper into it.
Proprioception in a nut shell is knowing where your body part is. For example where your arm is in relation to your body.
Practical example-
Close your eyes , and now using one hand touch the tip of your nose-
Congratulations, that’s one simple example of proprioception.
Any injury can impair a person’s proprioception at a joint and can be a risk factor for injuries to repeat themselves once muscular strength and range of movement has been restored.
Injury to a joint can cause direct or indirect alterations in regards to sensory information provided by mechanoreceptors.
Direct trauma- this can be from the spraining of a ligament and rupturing nerve fibres as they have less tensile strength than collagen. This reduction in nerve fibres can lead to a loss in proprioception.
Indirect- An example of this could be joint swelling, this would cause incorrect information to be relayed to the brain due to the change in pressure stimulating the receptors.
Proprioception exercises help your body regain control of the injured or impaired joint by helping control it. It helps to develop control at a subconscious level which is important in everyday activities as well as the sporting environment.
The most common piece of equipment would be the wobble board- This helps improve ankle and knee proprioception after an ankle sprain.
So there you go, a little bit more information on proprioception!!
Laskowski, E. R., Newcomer-Aney, K., & Smith, J. (1997). Refining rehabilitation with proprioception training: expediting return to play. The physician and sportsmedicine, 25(10), 89-102.
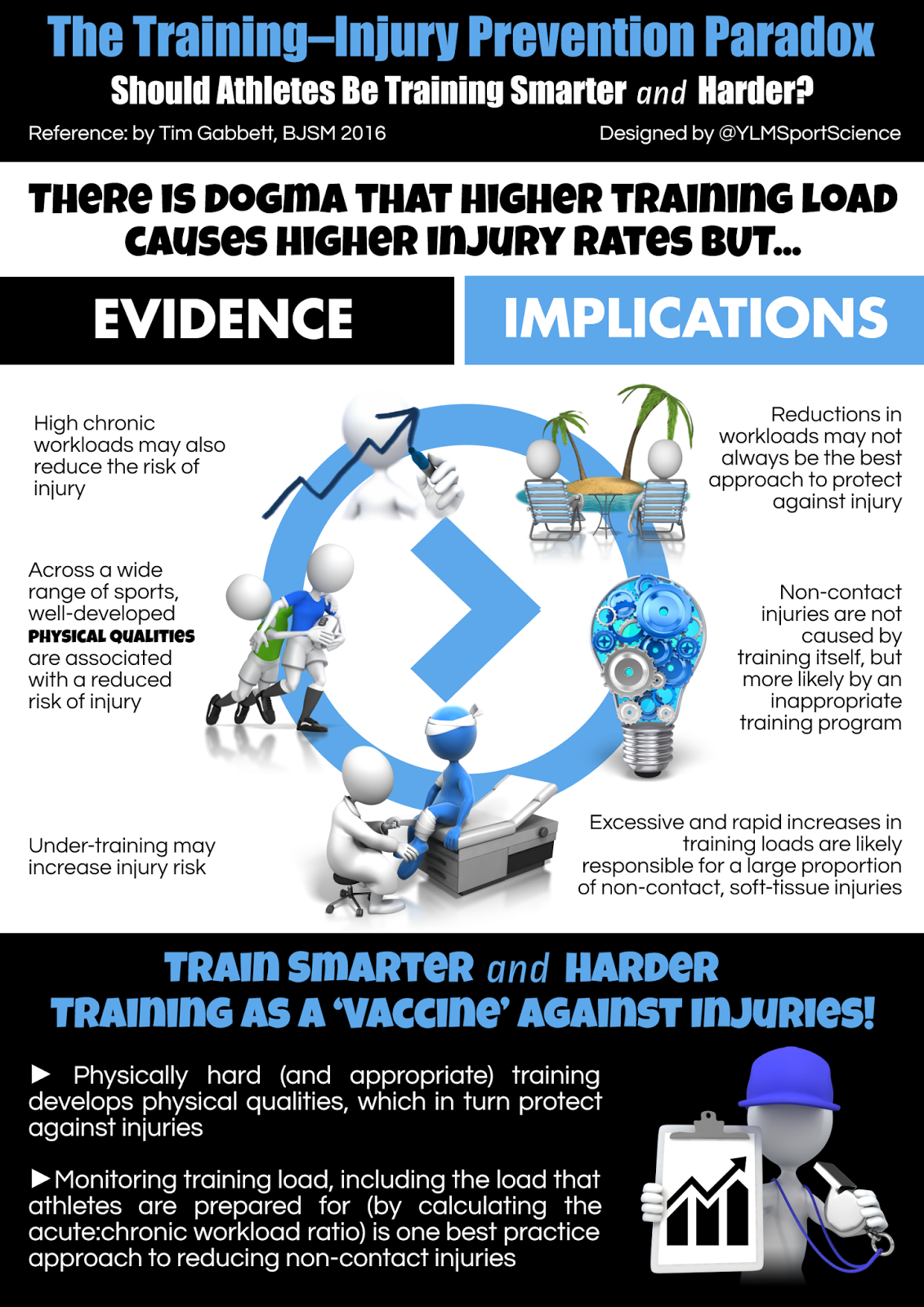
Training load related injuries are seen as ‘preventable’ injuries in the health care world.
High intensity training intensity + High volume = increased performance
This is excellent right? Well……
There is a need to balance the two. This because training at too high an intensity and or higher volume can lead to injury.
*Added to this it has also been found that too little training can also increase injury rate.
A 10% or more increase in training load can increase the injury risk from between 21% and 40% if however you increase a training load between 5 and 10% the injury rick lessens to 10% or less. This means there is a real need for coaches to monitor athletes loads High chronic work loads have been found to decrease the injury risk.
The double edged sword of all this is that across a wide range of sports, well-developed physical qualities are associated with a reduced risk of injury.
For athletes to develop these physical capacities that provide a protective defence against injury, they must be prepared to train hard. Thus the importance of balancing training intensity!
Gabbett, T. J. (2016). The training-injury prevention paradox: should athletes be training smarter and harder?. British journal of sports medicine, bjsports-2015.
To celebrate New Years and your fitness resolutions, Fully Fit Therapy is offering half price on all sessions to both new and returning customers!
This means an hour session for only £15.00!
If you would like advice on goal setting for your new years resolutions here is a link to a previous post I wrote – https://fullyfittherapy.co.uk/2016/01/02/176/
If you’d rather, feel free to give me a ring or email about anything from goal setting to injury/exercise questions.
Intense exercise can cause muscle damage, nervous system fatigue and also inflammation of muscles. This in turn reduces a persons performance by making the muscles sore and reducing the muscles ability to function.
It is no uncommon for athletes to experience elevated muscle soreness and reductions in muscle function of up to 20% for several days after intense exercise.
Cold water immersion is said to help reduce the recovery time needed. It is claimed that the decreased recovery time is due to temperature and pressure changes during cold water immersion.
One mechanism of cold water immersion is that it is said to reduce blood flow to the muscles. The blood flow reduction is said to reduce cell inflammation which is closely linked to the sensation of pain as it reduces the osmotic pressure in the area.
The other proposed mechanism is due to a reduction in tissue temperature. This decrease is said to reduce enzyme activity and also reduce secondary cell death of the cells surrounding the damaged muscle.
It is important to mention that body composition has found to affect tissue cooling time. The more adipose (fat) tissue around the area that is trying to be cooled, the longer it takes.
Cold water Immersion has been found to alleviate DOMs at at 24,48,72 & 96 hours after post exercise. The immersion was found to help with DOMS after high intensity exercise for both 24 hours and 48 hours after high intensity exercise. It was also established that it helped improve the recovery of muscular power but not strength.
The important parts to take from the above are that:
• Having an ice cold bath will not stop DOM’s after strenuous exercise. It will however reduce the severity of it.
• The exact mechanism has not been pin pointed, the tissue temp and pressure changes are just hypothesises.
So there you go- If you have had a tough training session or workout. Don’t go and have a hot bath, run the cold tap, chuck some ice cubes in the frame and jump on in!
Leeder, J., Gissane, C., van Someren, K., Gregson, W., & Howatson, G. (2011). Cold water immersion and recovery from strenuous exercise: a meta-analysis. British journal of sports medicine, bjsports-2011.
Most people these days have heard of an MRI scan or even had one done. They can be a useful tool for physicians to pick up an array of conditions and diseases.
One of the things you can get a scan for is of your back. This is what many people ask for relatively early on if not straight away when they get any sort of back pain.
Now a scan is very good at picking up abnormalities in the spine from bulges, protrusions and extrusions.
Now patient x has had lower back pain for a while and finally thinks they should go and have an MRI scan to see whats going on.
So patient x goes for a scan on their back and it turns out they have a bulging disc!
Patient x then has the operation to fix it…. Shock horror!!, their back pain pain is still there! How could this be you ask? The MRI scan showed a bulging disk which was obviously causing patient x’s pain. They then went and had the operation to fix it!
What happened with our hypothetical subject?
Well studies on MRI scans of the back have been going on since the 80’s. It was in the early 90’s a famous study by Maureen C. Jensen, Michael N. Brant-Zawadzki, Nancy Obuchowski, Michael T. Modic, Dennis Malkasian, and Jeffrey S. Ross.
They looked at 98 asymptomatic people (Completely healthy) and got them all to have an MRI scan of their lower back
A massive 52% had a bulge at one level, 27% had a protusion and 38% had an abnormality at more than one level. The authors concluded that protrusions or bulges in people with lower back pain may frequently be coincidental.
Another study, this time of the cervical spine ( top third of your spine) in 2012. A Massive 1211 people were recruited from their 20’s right through to their 70’s, both males and females. The authors came to the same conclusion as 1994 that there is a relatively high prevalence of abnormal MRI findings in symptom free people.
A complete review of spinal degeneration in symptom free populations took place earlier this year and reached the same conclusion that image-based degenerative features are very likely down to aging and are in face unassociated with pain.
It is potentially massive the number of people over the years have gone on and had operations needlessly off the back of having MRI scans.
It can even add an awful amount of stress as it causes unnessassery worry all because people aren’t told that these changes/abnormal findings are a perfectly natural sign of aging much like getting grey hairs and wrinkles.
Brinjikji, W., Luetmer, P. H., Comstock, B., Bresnahan, B. W., Chen, L. E., Deyo, R. A., … & Jarvik, J. G. (2015). Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. American Journal of Neuroradiology, 36(4), 811-816. http://www.ncbi.nlm.nih.gov/pubmed/25430861
Jensen, M. C., Brant-Zawadzki, M. N., Obuchowski, N., Modic, M. T., Malkasian, D., & Ross, J. S. (1994). Magnetic resonance imaging of the lumbar spine in people without back pain. New England Journal of Medicine, 331(2), 69-73.
Kato, F., Yukawa, Y., Suda, K., Yamagata, M., & Ueta, T. (2012). Normal morphology, age-related changes and abnormal findings of the cervical spine. Part II: Magnetic resonance imaging of over 1,200 asymptomatic subjects. European Spine Journal, 21(8), 1499-1507.
‘Am I pronating enough?’ ‘Am I pronating too much?!’ ‘Is that why I’m getting injured?’ Are questions runners have recently asked me when talking about their feet.
Studies seem to be saying a big resounding NO! pronation is not associated with an increase injury risk.
In fact some studies actually have concluded 7-10 degrees of pronation may be an advantage! SO don’t go thinking you need to aim for neutral!
Why do people have a view that pronation is bad and increases injury risk?!
Well the most likely explanation is down to marketing from shoe companies labelling pronation as harmful and providing a solution which is normally a very expensive shoe aiming to correct something that was never an issue!
Shoe companies may claim that their products help reduce injury risk but to date there is no evidence that supports this.
Sales>science.
Comfort has now been found to be a factor in determining injury risk.
If you had gone out and bought a new pair of shoes based on the fact you thought it was going to ‘correct’ an issue you had with your foot and persevered with using it. You are more than likely doing more harm to yourself!
In a study- 106 participants were told to pick the most comfortable shoe insert.
There were 6 to pick from and 5 were seen as the most preferred (picked at roughly the same frequency)
After being left to train for 4 months against a control group, the test group ended up having 53% less lower extremity injuries!
So there you go, don’t worry about finding the perfect angle or worrying about correcting your foot. Just go out and pick what shoe feels most comfortable for you!!
To have a look at the journals in this post go to:
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.OkNoRead more